EX-99.3
Published on September 27, 2022
|
Computershare Trust Company, N.A. PO Box 43006 Prov idence, RI 02940 - 3006 Within USA, US territories & Canada 866 249 2610 Outside USA, US territories & Canada 201 680 6578 www.computershare.com/investor Name Address City, State, Zip Holder Account Number — — — — — — — — — — — — — — Use a black pen. Print in CAPITAL letters inside the grey areas as shown in this example. This form is to be used for recurring debits only. Do not use for one time purchases. Direct Stock Purchase Plan - Direct Debit Authorization - Monthly Funds will be withdrawn on the 2 3rd day of the month or on the next business day. Dollar Amount: This plan allows for a minimum amount of $50 with a maximum of $10,000 per month. If applicable, an enrollment fee will be deducted from the initial investment. Financial Institution Information A. Please select one. Individual Joint Other B. Please select one. Checking Account Savings Account Financial institution account number Financial institution routing number Note: DO NOT USE A CREDIT CARD. If you do not know your account number or the routing number, please see the reverse side of this form or check with your financial institution. Account numbers must be in numeric format. Name(s) in which the above account is held Note: If you are not currently enrolled in this company’s Plan, by signing this form, you agree to the following: (1) to enro ll in the Plan for full dividend reinvestment so that all of your dividends will be u sed to purchase additional shares (if available); (2) to be bound by the terms and conditions of the prospectus or brochure that governs the Plan; (3) that you have read and fully understand the ter ms and conditions of the prospectus or brochure; and (4) t hat you further agree that your participation in the Plan will continue until you notify |
|
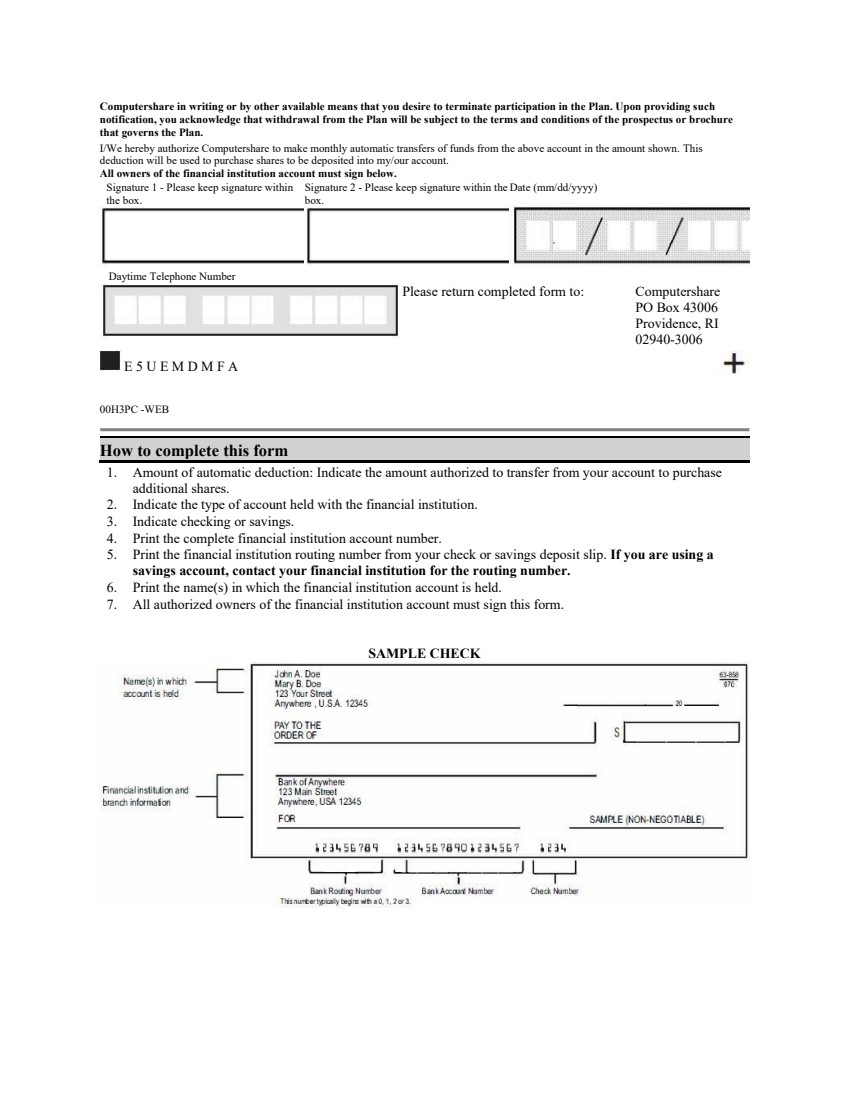
Computershare in writing or by other available means that you desire to terminate participation in the Plan. Upon providing s uch notification, you acknowledge that wit hdrawal from the Plan will be subject to the terms and conditions of the prospectus or brochure that governs the Plan. I/We hereby authorize Computershare to make monthly automatic transfers of funds from the above account in the amount shown. This deduct ion will be used to purchase shares to be deposited into my/our account. All owners of the financial institution account must sign below. Signature 1 - Please keep signature within the box. Signature 2 - Please keep signature within the box. Date (mm/dd/yyyy) Daytime Telephone Number Please return completed form to: Computershare PO Box 43006 Providence, RI 02940 - 3006 E 5 U E M D M F A 00H3PC - WEB How to complete this form 1. Amount of automatic deduction: Indicate the amount authorized to transfer from your account to purchase additional shares. 2. Indicate the type of account held with the financial institution. 3. Indicate checking or savings. 4. Print the comple te financial institution account number. 5. Print the financial institution routing number from your check or savings deposit slip. If you are using a savings account, contact your financial institution for the routing number. 6. Print the name(s) in which the financial institution account is held. 7. All authorized owners of the financial institution account must sign this form. SAMPLE CHECK |
|
6UEMD_00H3QA (Rev. 7/15) - WEB |
